The Impact of the New CVD Guidelines on RDNs and Other Health Professionals
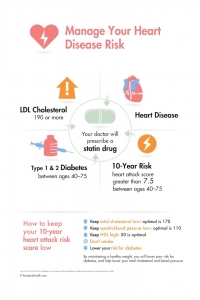
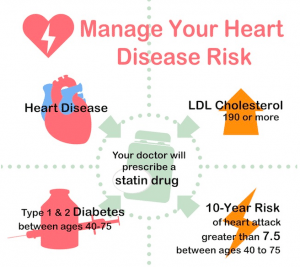 The 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults released in November 2013 strongly states that lifestyle is the foundation for atherosclerotic cardiovascular disease (ASCVD) risk reduction. Adhering to a heart healthy diet, getting regular exercise, avoiding tobacco products, and maintaining a healthy weight are key strategies for everyone. Even with statin therapy, lifestyle changes in food choices and physical activity levels are the cornerstone of primary and secondary prevention of ASCVD.With the advent of the new ASCVD risk calculator and the potential for a greater number of people to be placed on statin therapy, more people may be interested in learning how to lower low density lipoprotein cholesterol (LDL-C) levels and reduce overall risk with lifestyle changes as a way to avoid medication.The risk calculator includes four areas where diet plays a key role: total cholesterol, high density lipoprotein cholesterol (HDL-C), systolic blood pressure and diabetes. I suggest including gestational diabetes, pre-diabetes, and a family history of diabetes in the discussion. Although BMI is not included in the risk assessment calculator, a separate workgroup published guidelines on overweight and obesity as a part of the overall recommendations.The specific dietary changes are not new information, but instead reflect the body of research currently available. Recommendations were derived from high-quality randomized trials, meta-analyses, and observational studies. They were not formulated when sufficient evidence was not available. There is insufficient evidence to support dietary changes to lower total cholesterol -- instead the emphasis is on lowering LDL-C.The cornerstone of dietary recommendations to lower both LDL-C and blood pressure is to consume a diet that emphasizes intake of vegetables, fruits and whole grains; includes low-fat dairy products, poultry, fish, legumes, non-tropical vegetable oils and nuts; and limited intake of sweets, sugar-sweetened beverages and red meats. In addition, specific recommendations that received the strongest level of support include:To lower LDL-C:
The 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults released in November 2013 strongly states that lifestyle is the foundation for atherosclerotic cardiovascular disease (ASCVD) risk reduction. Adhering to a heart healthy diet, getting regular exercise, avoiding tobacco products, and maintaining a healthy weight are key strategies for everyone. Even with statin therapy, lifestyle changes in food choices and physical activity levels are the cornerstone of primary and secondary prevention of ASCVD.With the advent of the new ASCVD risk calculator and the potential for a greater number of people to be placed on statin therapy, more people may be interested in learning how to lower low density lipoprotein cholesterol (LDL-C) levels and reduce overall risk with lifestyle changes as a way to avoid medication.The risk calculator includes four areas where diet plays a key role: total cholesterol, high density lipoprotein cholesterol (HDL-C), systolic blood pressure and diabetes. I suggest including gestational diabetes, pre-diabetes, and a family history of diabetes in the discussion. Although BMI is not included in the risk assessment calculator, a separate workgroup published guidelines on overweight and obesity as a part of the overall recommendations.The specific dietary changes are not new information, but instead reflect the body of research currently available. Recommendations were derived from high-quality randomized trials, meta-analyses, and observational studies. They were not formulated when sufficient evidence was not available. There is insufficient evidence to support dietary changes to lower total cholesterol -- instead the emphasis is on lowering LDL-C.The cornerstone of dietary recommendations to lower both LDL-C and blood pressure is to consume a diet that emphasizes intake of vegetables, fruits and whole grains; includes low-fat dairy products, poultry, fish, legumes, non-tropical vegetable oils and nuts; and limited intake of sweets, sugar-sweetened beverages and red meats. In addition, specific recommendations that received the strongest level of support include:To lower LDL-C:
- Follow established and well-known plans like the DASH diet, the USDA Food Pattern, or the AHA Diet to achieve the suggested dietary pattern.
- A target of 5-6% of calories from saturated fat. Favorable effects on lipid profiles are greater when saturated fat is replaced by polyunsaturated fatty acids(PUFAs), followed by monounsaturated fatty acids (MOFAs), then whole grains.
- Reduce trans fat intake.
To lower blood pressure:
- Decrease sodium intake to 2400mg/day; further reduction to 1500mg/day is more helpful. A key is that some sodium reduction is beneficial, even if specific targets aren't reached. The report recommends at a minimum reducing sodium intake by 1000mg/day.
- These goals can be achieved with the DASH diet, combined with a decreased sodium intake.
Recommendations for physical activity encourage 3-4 moderate-to-vigorous intensity aerobic exercise sessions per week. The 'some is better than none' recommendation also applies to exercise and additional benefits occur as the amount of physical activity increases through higher intensity, greater frequency, and/or longer duration. The Physical Activity Toolkit is a comprehensive resource designed for registered dietitians (RDNs) to use with clients as part of the American College of Sports Medicine's "Exercise is Medicine" campaign.Specific recommendations from the overweight and obesity work group include:
- Use the current body mass index (BMI) cut point for overweight (BMI >25.0-29.9 kg/m2) and obesity (BMI of greater than or equal to 30 kg/m2) to identify adults who may be at elevated risk of cardiovascular disease (CVD), and the current cut point for obesity (BMI equal to or greater than 30) to identify adults who may be at elevated risk of mortality from all causes.
- Advise overweight and obese adults that the greater the BMI, the greater the risk of CVD, type 2 diabetes, and all-cause mortality.
- Advise adults that the greater the waist circumference, the greater the risk of CVD, type 2 diabetes, and all-cause mortality. The cut points currently in common use (>35 inches for women and >40 inches for men) may continue to be used to identify patients who may be at increased risk until further evidence becomes available.
- Sustained weight loss of 3-5% of total body weight is likely to result in clinically meaningful reductions in triglycerides, blood glucose, and the risk of developing type 2 diabetes.
- Greater amounts of weight loss will reduce blood pressure, improve ASCVD risk, and reduce the need for medication to control blood pressure, blood glucose and lipids, as well as further reduce triglycerides and blood glucose.
The report clearly states that adapting these recommendations to fit each person's individual calorie requirements, personal and cultural food preferences, and medical nutrition therapy for other conditions is required. There is no 'one-size-fits-all' recommendation, which makes it imperative for each person to work with a RDN to develop the most appropriate and effective plan for their individual situation.Publication of the new ASCVD guidelines present an important opportunity for RDNs to take the lead in providing lifestyle change programs that meet each individual person's need along with evaluating these programs. RDNs can also conduct research to further knowledge about best practices.References:
- 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology Foundation/ American Heart Association Task Force on Practice Guidelines. Circulation. 2013; 128: e240-e327.
- Eckel RH, Jakicic JM, Ard JD, Miller NH, Hubbard VS, Nonas CA, de Jesus JM, Sacks FM, Lee I-M, Smith Jr SC, Lichtenstein AH, Svetkey LP, Loria CM, Wadden TW, Millen BE, Yanovski SZ, 2013 AHA/ACC Guideline on Lifestyle Management to Reduce Cardiovascular Risk, Journal of the American College of Cardiology (2013), doi: 10.1016/j.jacc.2013.11.003.
- Assessing your weight and health risk. NIH/NHLBI. http://www.nhlbi.nih.gov/health/public/heart/obesity/lose_wt/risk.htm.
- 2013 Prevention Guidelines Tools. CV Risk Calculator. http://my.americanheart.org/professional/StatementsGuidelines/PreventionGuidelines/Prevention-Guidelines_UCM_457698_SubHomePage.jsp.
By Lynne Grieger, RDN, CDE, CPTWe've been working around the clock to get the best heart health and cholesterol resources to you. They're great resources for your clients and are chock-full of the latest scientific data. View the full selection at the Nutrition Education Store, or browse the top sellers below...